Approaches
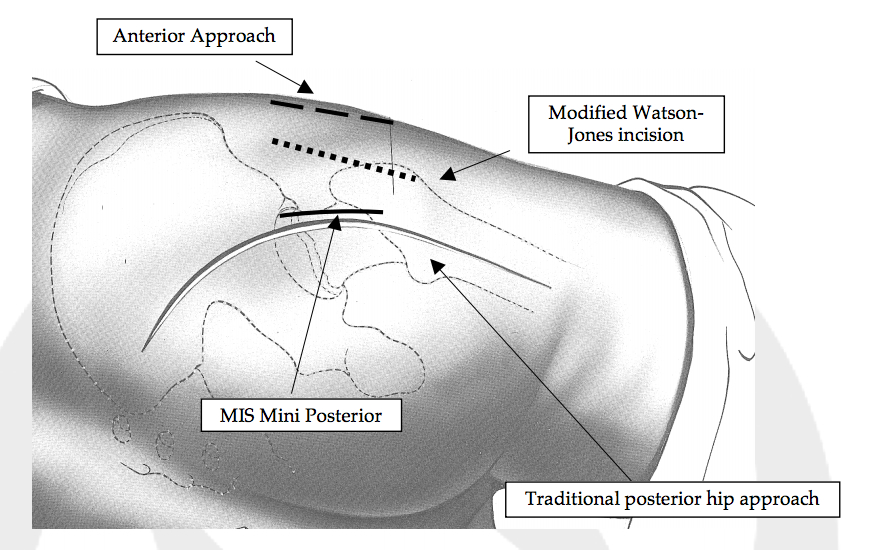
Over time, many different surgical approaches have been explored, each with its own specific advantages and disadvantages. The lateral, or side, hip surgical approach historically involved a controlled fracture (osteotomy) of the trochanter including the insertion of the hip abductor muscles (analogous to the rotator cuff of the shoulder). This required bone reattachment which carried associated risks of improper bone healing and a postoperative limp. An anterolateral, slightly more anterior, approach avoided bone osteotomy, but instead detaches the anterior third of the hip abductor muscle off of the bone. While the approach provides excellent hip stability, it also leads to at least a temporary limp, because of the dissection through the hip abductor musculature. An approach again just slightly forward to this one, a modified Watson-Jones anterolateral approach, promotes many of the same advantages, and avoids abductor damage because it enters the hip joint just in front of this muscle group. However, the technique is challenging for exposure in the operating room, requiring multiple assistants and extensive leg manipulation. Because exposure is more difficult, it can be more challenging for accurate component placement. I have performed all of these approaches, but have found the advantages to not be as great as other surgical techniques.
The mini-posterior approach is a modification of the standard posterior hip surgical technique. In contrast to the standard posterior approach, this technique leaves more muscle and soft tissue intact, and the cut tendons and capsule are repaired at the end of the case. However, muscle is required to be cut and repaired to perform this approach. Repair lowers the hip dislocation rate to be comparable to the other standard approaches, but not as low as the anterior approach. Because this modified approach is based on the traditional posterior technique, it is extensile if needed, thereby allowing appropriate hip exposure in the rare occurrence of an intraoperative complication, unexpected complex hip anatomy, or revision procedures. Hip precautions are recommended after surgery for 6 weeks, and hip instability can occur early or late after surgery.
An anterior hip approach is unique in that it is muscle-splitting rather than cutting, as opposed to the other approaches, and consequently has fewer precautions after surgery. As this surgical approach has gained popularity, it has recently become the predominant surgical approach used in the United States because of its inherent advantages over traditional approaches. Increasing research and studies have shown that reduced pain, no hip precautions, better hip stability, more accurate implant placement, and faster recovery can be reliably reproduced by surgeon experts. A major advantage of this technique is the ability to use xray throughout the procedure to optimize implant size and position, and to match leg lengths (all other approaches use xray only in the recovery room after surgery is complete).
I have been trained in this technique by Dr. Joel Matta, and use this approach for over 95% of my patients. In some cases, like revision surgery or complex hip replacement, a posterior approach can be beneficial. But for first-time hip replacement, anterior hip replacement has shown significant advantages over the older approaches. I am the only surgeon at the Institute currently performing anterior hip replacement, and in fact, the only surgeon to have ever performed it at the Institute. In my experience, patients have less pain and a faster recovery with this surgical technique. Patients routinely are able to go home the same day of surgery or the following morning safely. Discussing this approach with a surgeon who actively performs the procedure would best be able to explain advantages of anterior hip replacement.